




Trial Designs
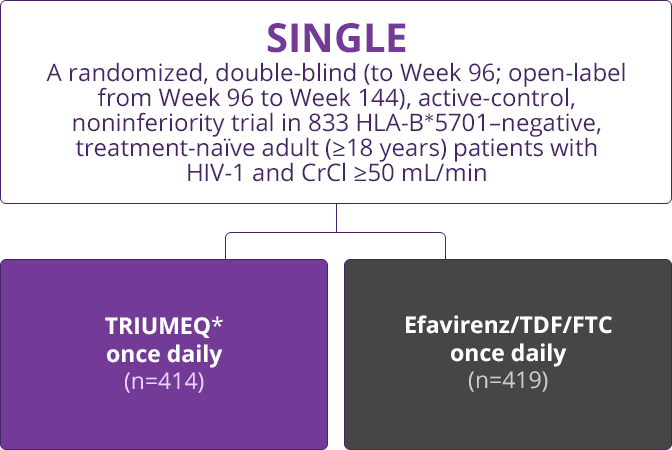
TRIUMEQ in the SINGLE Trial1
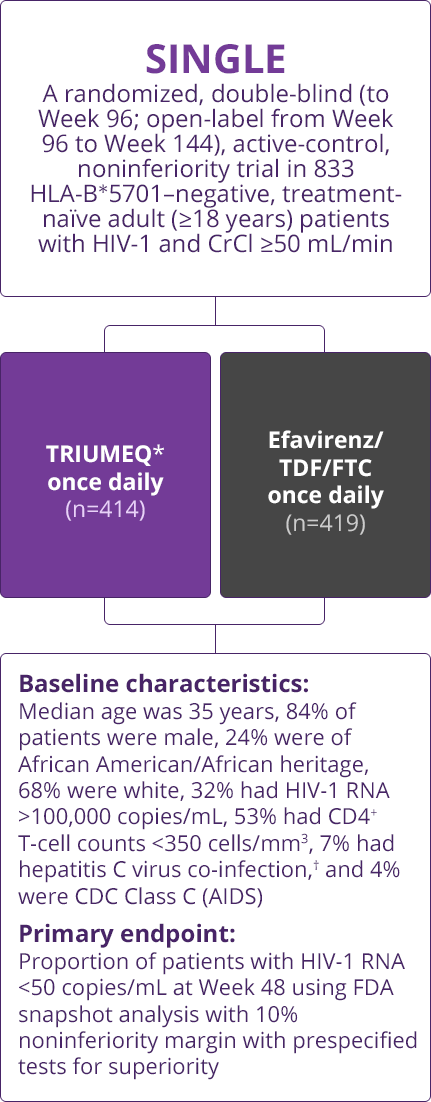
- Baseline characteristics: Median age was 35 years, 84% of patients were male, 24% were of African American/African heritage, 68% were white, 32% had HIV-1 RNA >100,000 copies/mL, 53% had CD4+ T-cell counts <350 cells/mm3, 7% had hepatitis C virus co-infection,† and 4% were CDC Class C (AIDS)
- Primary endpoint: Proportion of patients with HIV-1 RNA <50 copies/mL at Week 48 using FDA snapshot analysis with 10% noninferiority margin with prespecified tests for superiority
✶Patients received 1 dolutegravir 50-mg tablet and fixed-dose ABC/3TC. This regimen is bioequivalent to 1 TRIUMEQ tablet under fasted conditions.
†Hepatitis B virus co-infection was an exclusion criterion.
CrCl=creatinine clearance; TDF/FTC=tenofovir/emtricitabine; CDC=Centers for Disease Control and Prevention; ABC/3TC=abacavir/lamivudine.
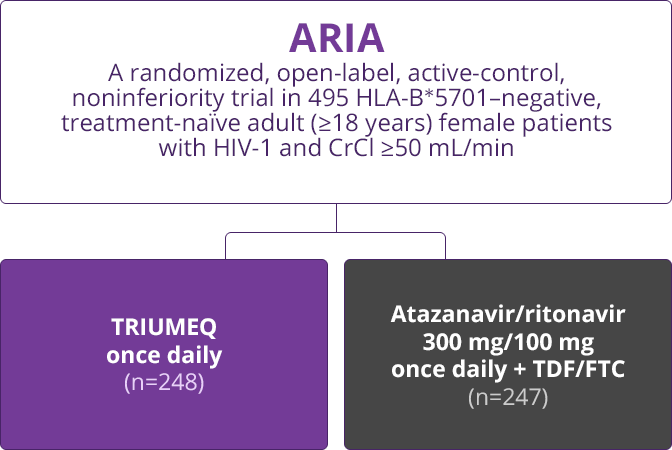
TRIUMEQ in the ARIA Trial2
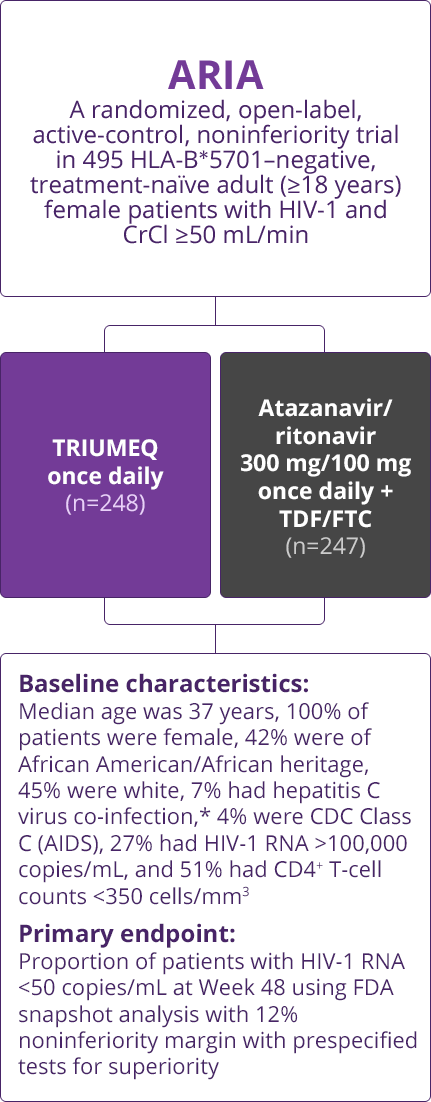
- Baseline characteristics: Median age was 37 years, 100% of patients were female, 42% were of African American/African heritage, 45% were white, 7% had hepatitis C virus co-infection,*4% were CDC Class C (AIDS), 27% had HIV-1 RNA >100,000 copies/mL, and 51% had CD4+ T-cell counts <350 cells/mm3
- Primary endpoint: Proportion of patients with HIV-1 RNA <50 copies/mL at Week 48 using FDA snapshot analysis with 12% noninferiority margin with prespecified tests for superiority
✶Hepatitis B virus co-infection was an exclusion criterion.
CrCl=creatinine clearance; TDF/FTC=tenofovir/emtricitabine; CDC=Centers for Disease Control and Prevention.

Virologic Response
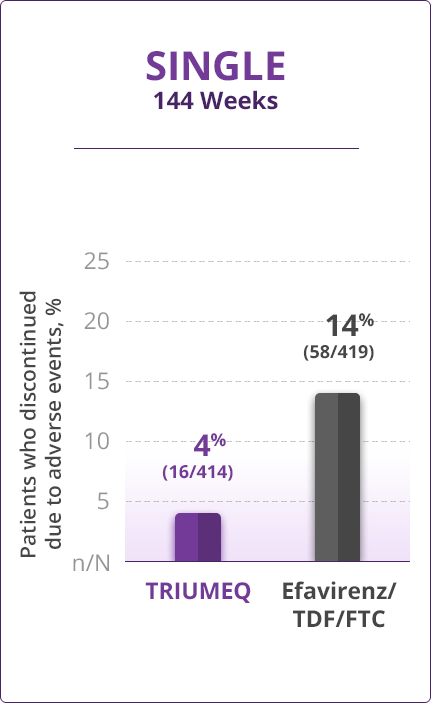
Statistically superior long-term result with TRIUMEQ vs efavirenz/TDF/FTC at week 1441,3
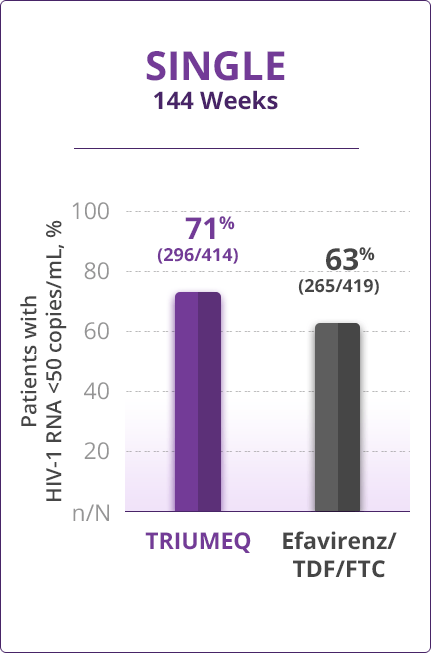
- Treatment difference (8.3% [95% CI; 2.0%, 14.6%]) was driven primarily by rates of discontinuation due to adverse events (4% for TRIUMEQ vs 14% for efavirenz/TDF/FTC)
Booster-free TRIUMEQ showed a statistically superior virologic response at 48 weeks vs a regimen with atazanavir/ritonavir2,3
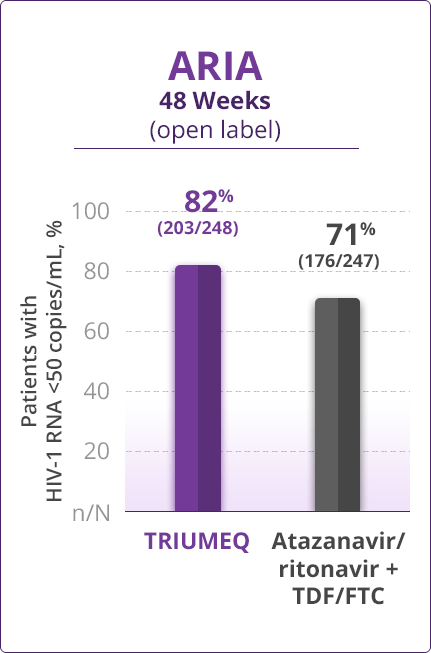
- Treatment difference (10.5% [95% CI; 3.1%, 17.8%]) was driven primarily by a lower rate of virologic nonresponse (6% for TRIUMEQ vs 14% for atazanavir/ritonavir + TDF/FTC) and discontinuations due to adverse events or death (4% and 7%, respectively)
- Direct comparisons across trials should not be made due to differing trial designs

Resistance Results
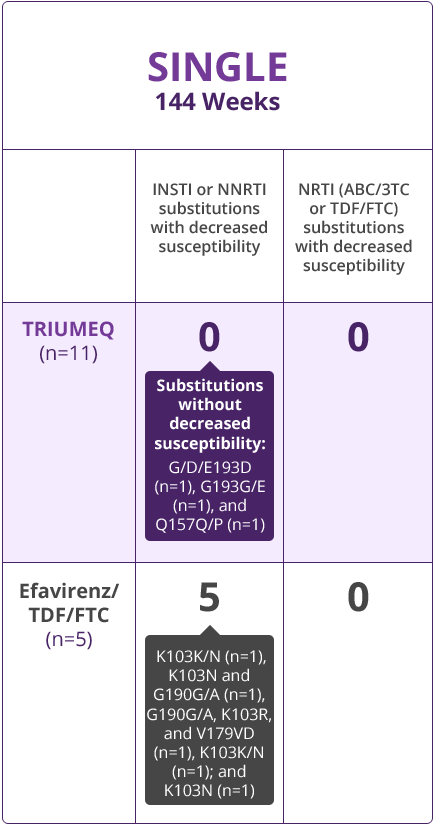
144-Week Results From the SINGLE Trial Support a High Barrier to Resistance With TRIUMEQ3
In SINGLE, no patients receiving TRIUMEQ had detectable decreases in susceptibility to the components of TRIUMEQ (dolutegravir, abacavir, or lamivudine) in the resistance analysis data set (n=11 with confirmed HIV-1 RNA >400 copies/mL at failure or last visit and having resistance data).
Number of patients with treatment-emergent INSTI, NNRTI, or NRTI substitutions with decreased susceptibility to ARVs studied based on the resistance analysis data set through 144 weeks3
INSTI=integrase strand transfer inhibitor; NNRTI=non-nucleoside reverse transcriptase inhibitor; NRTI=nucleoside reverse transcriptase inhibitor; ARV=antiretroviral.
- While there were no detectable decreases in susceptibility to the components of TRIUMEQ (abacavir, dolutegravir, or lamivudine), 2 patients with virologic failure assigned to TRIUMEQ had treatment-emergent G/D/E193D and G193G/E integrase substitutions at Week 84 and Week 108, respectively, and 1 subject with 275 copies/mL HIV-1 RNA had a treatment-emergent Q157Q/P integrase substitution detected at Week 24
48-Week Results From the ARIA Trial Support a High Barrier to Resistance With TRIUMEQ3
In ARIA, no patients receiving TRIUMEQ had detectable decreases in susceptibility to the components of TRIUMEQ (abacavir, dolutegravir, or lamivudine) in the resistance analysis data set (n=6 with 2 consecutive assessments of plasma HIV-1 RNA ≥400 copies/mL at failure or last visit and having resistance data).
Number of patients with treatment-emergent INSTI, PI, or NRTI substitutions with decreased susceptibility to ARVs studied based on the resistance analysis data set through 48 weeks3
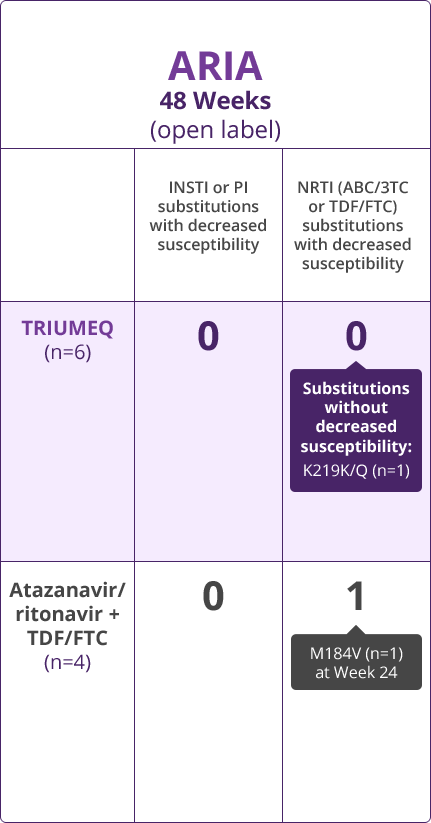
INSTI=integrase strand transfer inhibitor; PI=protease inhibitor; NRTI=nucleoside reverse transcriptase inhibitor; ARV=antiretroviral.
- Direct comparisons across trials should not be made due to differing trial designs

Discontinuations Due to AEs
Proportion of patients who discontinued due to adverse events1,3
Proportion of patients who discontinued due to adverse events2,3
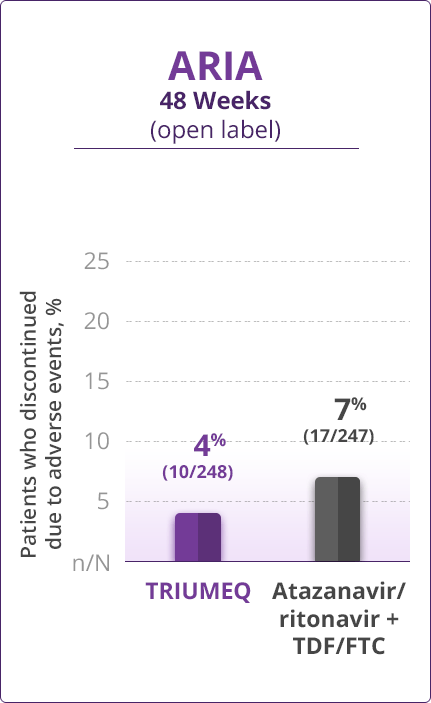
- Direct comparisons across trials should not be made due to differing trial designs
Adverse Drug Reactions (ADRs)
Grades 2 to 4 treatment-emergent ADRs (≥2% frequency)3
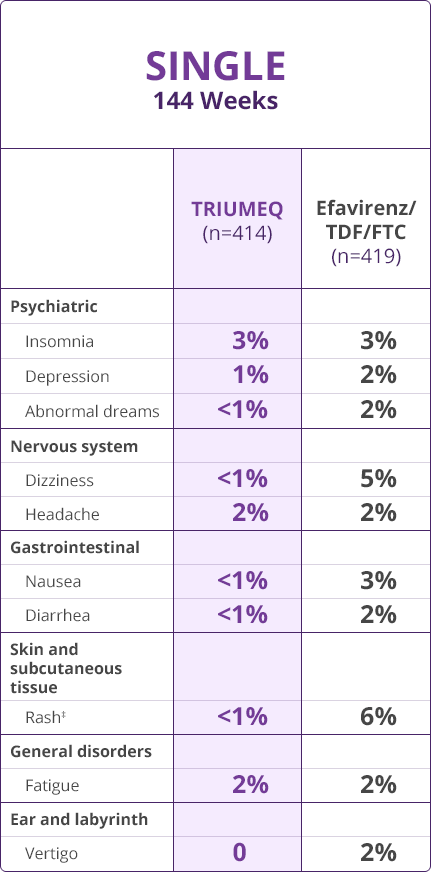
Grade 1 insomnia rates:
- 7% and 4% in patients receiving TRIUMEQ and efavirenz/TDF/FTC, respectively
‡Includes pooled terms: rash, rash generalized, rash macular, rash maculopapular, rash pruritic, and drug eruption.
Grades 2 to 4 treatment-emergent ADRs (≥2% frequency)3
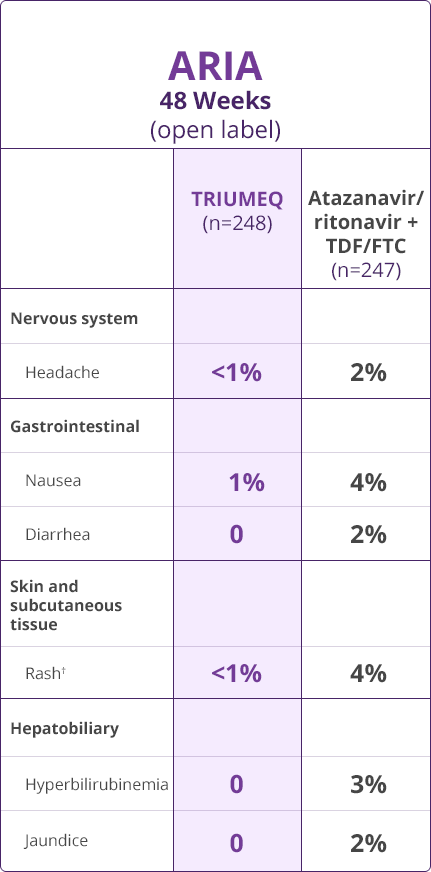
†Includes rash, rash generalized, rash maculopapular, rash papular; and rash pruritic.
- Direct comparisons across trials should not be made due to differing trial designs
Please see full Prescribing Information, including Boxed Warning and Medication Guide, for TRIUMEQ and TRIUMEQ PD.
References
- Walmsley S, Baumgarten A, Berenguer J, et al. Dolutegravir plus abacavir/lamivudine for the treatment of HIV-1 infection in antiretroviral therapy-naive patients: week 96 and week 144 results from the SINGLE randomized clinical trial. J Acquir Immune Defic Syndr. 2015;70(5):515-519.
- Orrell C, Hagins DP, Belonosova E, et al; on behalf of the ARIA Study Team. Fixed-dose combination dolutegravir, abacavir, and lamivudine versus ritonavir-boosted atazanavir plus tenofovir disoproxil fumarate and emtricitabine in previously untreated women with HIV-1 infection (ARIA): week 48 results from a randomised, open-label, non-inferiority, phase 3 study. Lancet HIV. 2017;4(12):e536-e546.
- Data on file, ViiV Healthcare.
DALWCNT220006